In October 2010 The UK Department of International Development (DFID) approved a proposal submitted by Help the Hospices to work with ICPCN to improve access to palliative care for children with HIV/AIDS in Malawi and the Maharashtra District of India, over a five year period. The ICPCN is acting as the co-ordinating body to enhance support in the development of children's palliative care programmes in these two countries.
News and updates on the DFID 2 country project
News from Malawi - April 2013
MEETING OF CHILDREN LIVING WITH LIFE LIMITING ILLNESSES AND THE POLICY MAKERS ON 26TH MARCH 2013.
It was on 26th March 2013 when Children's Palliative Care (CPC) project under the
It was on 26th March 2013 when Children's Palliative Care (CPC) project under the
Palliative Care Association of Malawi (
PACAM) organised and hosted a meeting between the children living with life limiting illnesses and the policy makers. The guest of honour at this meeting was the Minster of Health, Honourable Catherine Gotani Hara.
PACAM) organised and hosted a meeting between the children living with life limiting illnesses and the policy makers. The guest of honour at this meeting was the Minster of Health, Honourable Catherine Gotani Hara.
It was an exciting moment when the children were told that the meeting they longed for had finally been scheduled and accepted to take place. Each one of them wanted to be there and speak with the minister but due to financial challenges only a few were represented.
It was all smiles when the Minister of health entered the meeting hall as the children now believed that it was happening.
The meeting started at 10h00 with a prayer and the speeches from the national coordinator of the PACAM, Mr Lameck Thambo. In his speech he gave a brief background of PACAM, the CPC project and various activities done by PACAM and the project.
This was followed by the voices of children who came up with issues like drug shortages, lack of clinic space, toys and play areas, need of nutritional support, having too few trained CPC service providers resulting in long waiting time at the clinics, lack of teachers to help those children who stay long in the hospital so that they do not miss out on classes, special teachers in schools for slow learners due to illnesses and lack of specialised children's palliative care centres among others.
In her speech the minister promised that her ministry will ensure that the drugs, especially pain relieving medications like morphine and others are always available in hospitals, she also promised to work with other organisations in sourcing nutrition supplements for children with life limiting illnesses and to train more CPC service providers to curb shortage of skilled CPC service providers.
Below are some of the pictures from the meeting. The first picture shows some of the children who attended the meeting, the second the table of dignitaries and the third a child talking to the participants of the meeting.



News from Malawi - March 2013
EMPOWERMENT WORKSHOPS AND FOCUS GROUP DISCUSSIONS
Empowerment workshops for children with life limiting illnesses are one of the activities which enable them to meet and share experiences. It helps them to learn more about their various illnesses and ways to cope.
This is also the same with parents who may have been suffering for some timeor have challenges they did not have the solutions for. The main objectives of these workshops and focus group discussions are:
- To sensitise children to children’s palliative care.
- To create awareness of palliative care services available to children of Malawi.
- To make them aware of their rights regarding palliative care.
- To create an environment where children who face life limiting and life threatening conditions will be able to share their experiences and be able to advocate for their needs.
The activities during these gatherings include sessions on different topics such as life-limiting illnesses, nutrition, psychosocial care, rights of children with life limiting illnesses according to the ICPCN charter, sickle cell disease, epilepsy, cerebral palsy, drugs used in palliative care and many more as requested by either the children themselves or their guardians.
In Malawi, empowerment workshops and focus group discussions are ongoing and each site conducts one workshop and focus group discussion in each quarter.
These discussions provide an environment where children with life limiting conditions and their guardians can share their experiences, learn from each other and from service providers, share challenges and help each other with ideas on how they can overcome them. Focus group discussions help them to air their concerns, give their opinions about the services and channel them to the appropriate people for consideration. They also act as a support group for the children and guardians.
However these workshops and focus group discussions come with challenges such as transport costs since some people come from far. It could have been better if these activities can be conducted at centres close to their homes.


Advocacy
In October last year we had a visit by Busi Nkosi, the ICPCN’s advocacy officer based in South Africa, to help us with advocacy issues. While in Malawi, she visited some government and non-governmental offices to find out about CPC activities and advocate for the services where they have not been started. Among the sites she visited were the nurses and midwives council of Malawi, Catholic health commission, National association of people living with HIV/AIDS and Kamuzu Central Hospital’s children’s palliative care clinic.
It was this visit which stimulated the nurses and midwives council to include CPC into the nursing curriculum which they are currently working on with the help of the Palliative Care Association of Malawi (PACAM) and the Ministry of Health. The visit also taught us that advocacy does not necessarily need a big gathering of people – a one-to-one talk can also make a difference. Busi, we are so grateful for your visit.
Meeting with National Associations
 PACAM held a meeting with the national associations based in Lilongwe. These are the associations which are mainly involved in HIV /AIDS activities. We were privileged during this meeting to have a police officer who is responsible for child protection who spoke about the child protection policy with the other participants.
PACAM held a meeting with the national associations based in Lilongwe. These are the associations which are mainly involved in HIV /AIDS activities. We were privileged during this meeting to have a police officer who is responsible for child protection who spoke about the child protection policy with the other participants.
The main objective of this meeting was to brief the associations about the Children’s Palliative Care (CPC) project, orient them on CPC activities, update them on the progress of the project and ask them to help in advocating for children’s palliative care services in their various associations.
During this meeting it was learnt that most of these organisations were at one point coming in contact with children with life-limiting illnesses but they did not know where to refer them. We hope that now they will be able to refer the children to the service provision sites.
The presence of the police officer responsible for child protection activities was a chance for PACAM to learn on how best to handle child protection issues and who to contact when a case of abuse comes up.
The participants promised to help in advocating for CPC in their organisations and through their various networks. They also promised to help in disseminating information about CPC through various means, including churches.
Mentorship visits
We have just had a mentorship visit of all the CPC sites by our local mentor, Umodzi. The objective of the visit was to interact with service providers and follow up on activities which have been going on since the project started, checking on data, services provided and share ideas on the way forward.
During the visits, service providers shared their challenges such as lack of space, drug cupboards for stocking drugs especially morphine, lack of children’s toys and play facilities, erratic supply of some pain relieving medications in paediatric formulation. We shared with the providers tips on how to have an effective palliative care team and the composition of the team, how to collect data and general issues on how to manage patients.
All in all the visits were successful and all the management teams are supportive towards the CPC services. In all the sites there is at least a room used for CPC although some clinics are shared with other medical clinics which means that some days the clinics are not open.
Mentorship is important because it is one way to give support to service providers, reinforce the standards set, share knowledge and learn from each other.
Upcoming events
We are planning to have a meeting between children with life limiting illnesses and the policy makers this month end as a way of advocating for CPC at the same time to gain government commitment. Currently the processes are underway and we hope it will work out.
2012
Historic meeting of leads from both Malawi and India held in Cardiff in July

On Thursday 12 July a historic meeting was held in Cardiff when the leads from both the DFID 2 country project met together with Kate North from Help the Hospices and Joan Marston from ICPCN.
This was the first time the leads from each country had been given the opportunity to meet and compare both the progress and the challenges faced in their respective countries. During the Cardiff 2012 PPC Conference representatives from both countries were given the opportunity to share news on children's palliative care from their regions with delegates. Dr Pradnya Talawadeker was a plenary speaker and gave delegates a fascinating insight into the unique challenges and opportunities facing CPC practitioners in India.
Seated from left to right are: Mrs Jean Tauzie (Malawi); Dr Maryann Muckaden (TATA Memorial Hospital in India and ICPCN Board Trustee); Kate North (Help the Hospices); Lameck Thambo (Director of PACAM); Dr Pradnya Talawadeker (India) and Joan Marston (ICPCN Chief Executive)
The latest news from Malawi (June 2012)
PACAM is implementing the children’s palliative care project in the three referral hospitals of Zomba Mzuzu and Kamuzu Central Hospital. The project is funded by DFID through Help the Hospices with mentorship from ICPCN.PACAM conducted a needs assessment in all the three sites and it was found that the sites had a common challenge in data collection, storage and management. The sites therefore requested PACAM purchase computers which could help them in data processing for the project. Following this request PACAM purchased three sets of computers and printers to be used in these three sites.
PACAM embarked on the activity of donating these computers to the sites. The first computer was donated to Zomba central hospital on 11th May 2012, the second one was to Kamuzu central hospital on 24th May 2012 and the third one to Mzuzu central hospital on 8th June 2012.
The first donation which was at Zomba was done by the National coordinator who handed over the computer to the palliative care coordinator on behalf of the hospital director. In her speech, the coordinator thanked PACAM for the donation and promised to use the computer and the printer for the intended purpose.

KAMUZU CENTRAL HOSPITAL DONATION
The donation at Kamuzu central hospital was done by the trustee board chair who on behalf of PACAM handed over the computer set and printer to the Hospital director. In his acceptance speech, the director of Kamuzu central hospital welcomed the donation and said it had come at the time when the hospital needs it and at the time when the hospital is in the process of setting up the intranet. In his speech he also thanked PACAM for the donation and urged those who will be using the computer to use it accordingly.
Below the trustee chair is shaking hands with hospital director during the official handover of the computer while the CPC project leader looks on.

May 2012
 About 40 health care workers from district and mission hospitals from the north and central regions have been sensitised in CPC through community sensitisation and media campaign workshops and over 500 others through general palliative care meetings. Participants to these workshops were district Palliative care/Home based care coordinators from government district hospitals and mission hospitals and media representatives from community radios and Malawi news agency (MANA).
About 40 health care workers from district and mission hospitals from the north and central regions have been sensitised in CPC through community sensitisation and media campaign workshops and over 500 others through general palliative care meetings. Participants to these workshops were district Palliative care/Home based care coordinators from government district hospitals and mission hospitals and media representatives from community radios and Malawi news agency (MANA). 
The latest news from India
April 2013
- The Children's Palliative Care (CPC) Project in collaboration with the Department of Palliative Medicine, Tata Memorial Centre, Mumbai organized a 1 Day Workshop on Paediatric Palliative Care on 5 February, 2013. Around 90 participants (Paediatricians, Doctors, Nurses, Social workers and volunteers attended the workshop. The Workshop was conducted by a team of International Faculty. The workshop was a first step to creating awareness in CPC among health professionals in all fields.
- CPC has also launched its 1st Edition a “Training Manual on Paediatric Palliative Care” a tool and guide for Health Care Professionals working with Children and Families. This was formally inaugurated and released on 5 Feb, 2013.
- Dr. Mrunal Marathe, Counsellor CPC secured the 1st place in the oral presentation on "Understanding and awareness of a child regarding his/her life threatening/limiting conditions" represented at the IAPC CON Feb 2013 at Bangalore.
- Lokmanya Tilak Muncipal General Hospital, Sion has set up a separate Paediatric Palliative Care OPD which was inaugurated on 23 Feb, 2013 for providing Palliative Care to children with HIV and their families. Ongoing activities and FGD’s are conducted with children and caregivers.
- The Children’s Palliative Care (CPC) Project set up its OPD at the Mahatma Gandhi Mission Hospital (MGM), Kalamboli. This was formally inaugurated on Wednesday 13th March, 2013 by esteemed Representatives from the Medical Fraternity & Staff at MGM.
- Children with various conditions like Cardiac, Respiratory, Neurological illnesses, HIV, Thalassemia, CP, MR are following up with the hospital. This is a separate hospital unit at Kalamboli for Women and children established since 1990. The hospital also has a neonatal care unit with all the facilities. It has also a rural outreach programme.
- CPC has made a Documentary (20 Min Film) on Sensitizing Govt/ Stakeholders/ Health Professionals and general public to raise awareness about CPC. A short 2 min clip has also been prepared
- The Maharashtra State government comes up with Palliative Care Policy a detailed article has been published in the Indian Express on 13 March, 2013 about the Maharashtra Govt, Dept of Health to take up this initiative and support Palliative Care which is to be implemented in 6 districts through the NCD Program, currently Palliative Care is being implemented at Jawhar and Igatpuri through Refresher Trainings and Train the Trainers for all cadres – Doctors/ Nurses/ ANM’s & ASHA Workers. This has been achieved through ongoing facilitation and advocating with Govt. Officials at various levels at both State and Central level. The stakeholders meeting are arranged every quarterly to review the actions taken and plans for further interventions.
- (http://www.indianexpress.com/news/state-government-comes-up-with-palliative-care- policy/1087167/1)
- Meeting with Representatives from Ministry of Women & Child Welfare, has facilitated a proposal draft for a Sponsorship Scheme which has been approved for Children suffering with a Life Limiting illness for Supportive Care through Rehabilitation of children and Family, which shall be under the guidance of the Ministry of Women and Child Development. A sponsorship of Rs 1000/- per month per child and family shall be subject to the conditions laid down in the ICPS Implementation plan. This is the first scheme to be initiated in collaboration with a Hospital. This will be subsequently implemented in various other hospitals also.
- Children and families were empowered through Magic Show at Wadia & Sion conducted by a group of physically challenged. Awareness sessions were also conducted sensitizing parents about CPC.
- CPC as a model site was visited and observed by a group of Paediatricians from 25th – 28th March, 2013 from Assunta Palliative Care Centre (ASPACC), Malaysia
- ICPCN in collaboration with the Tata Memorial Centre, Parel Mumbai is hosting the 1st International Conference in India, Mumbai “Transforming Children Palliative Care from Ideas…to Actions” from 10 – 12 Feb, 2014.
Sites: A Service Delivery Approach
The following sites were identified for implementing Palliative Care
- Lokmanya Tilak Municipal General Hospital (L.T.M.G.H) Sion, Mumbai The Regional Paediatric AIDS Centre at LTMG Hospital is a national Centre of Excellence for Paediatric HIV and has around 1785 registered children. The aim is to provide Palliative Care with an holistic approach including Psycho-social care for Children with HIV. More than 40 children have been included in CPC and have been provided various types of interventions.
- Jawhar Cottage Rural Hospital,Thane: Meeting with the Health Minister of Maharashtra was instrumental in getting this site for training and awareness on CPC in the rural part of Maharashtra. The program is Community based. ASHA Workers of NRHM project act as a liason for referral of patients from community to PHC’s in collaboration. The doctors and Health care workers have been trained in Palliative Care
Advocacy for CPC by adoption of Paediatric Palliative Care Policy by the Government (Involvement of National & International Organizations & Health Ministry)
- Desk review of need and statistics for Childrens Palliative Care in Maharashtra is being done. The aim of the review is to find out the chronic disease burden in children, and the support, treatment and medicines available to them. A fact sheet on HIV in Maharashtra was prepared
- A draft of Maharashtra Palliative Care Policy was formulated with IAPC-Maharashtra for advocating with various government departments.It was presented to Mr Suresh Shetty, Minister for Health and Dr. Vijaykumar Gavit, Minister of Medical Education and Horticulture. Dr Gavit was requested to be a Champion for the cause.
- A meeting was held with Additional Municipal Commissioner Manisha Maiskar and Dr Sandhya Kamat,Dean,Sion Hospital for setting up Palliative Care Units in Municipal and Tertiary Care Centres.
- A meeting was held with Dr. Sandhya Kamat - Dean Sion Hospital and HODs from various departments of Sion Hospital to deliver Palliative Care as a Primary Care service as well as training of Doctors/ Health Care Workers.
- Various work groups have been formed for Advocacy. (With Dr Leena Gangoli and Dr Roy, BARC Hospital, Sion Pediatrics and other departments, Jawhar Cottage Hospital, Mr Manek Daver, Spenta Communication, NGOs).
- Co-ordination was done with Indian Association of Paediatrics (IAP) and Mumbai Academy of Paediatrics for CME Training in Palliative Care for Paediatricians in Childrens Palliative Care.
- Meetings with MDACS and MSACS were held to schedule Sensitisation Lectures, for Palliative Care in HIV for Counsellors and doctors.
- A draft of Child Protection Policy was presented to the Director of Tata Memorial Hospital.
- Press meeting was arranged with Dr. Muckaden, Ms.Joan Marston, Dr Anilkumar Paleri and Ms Kate Tattersal for emphasizing the current situation of Palliative Care for Children in India. An article was published in DNA newspaper on 15th Oct 2011.
- CPC Press Club Meeting was organised for creating Media awareness in CPC.
- 21 Journalists attended the Press Meeting. Articles were published in December 2011 in
- Loksatta, Lokmat and Pudari (Marathi) and in January 2012 in Midday.
- Awareness talk was delivered on Palliative Care concept for radio broadcasting. Talk was broadcasted on Akashvani- Asmita Channel on 19th December 2011.
Training and awareness to Doctors, Nurses, Social Workers, Health Care Professionals, Volunteers and NGO’s in Knowledge, attitude and skill to deliver supportive care to children:
- Training material for Jawhar (Rural Site) has been developed for creating community awareness.
- Case Record Forms for Sion and Jawhar based on Patient Demographics/ Social & Psychological Assessment/ Home Visit/ Clinical History/ Examination/ Nursing Assessment/ Follow – Up/ Intervention have been developed.
- Training for doctors and health care workers was conducted for Jawhar (Rural Site) .
- Indian Association of Palliative Care (IAPC) in collaboration with TMC conducted a Certificate Training Course in “ Essentials of Palliative Care” for Doctors and Nurses in June and November 2011.
- The Maharashtra Medical Council was co-ordinated for granting credit points for IAPC Training in Palliative Care with emphasis on Paediatric Palliative Care
- Community awareness was conducted in various parts of Mumbai in collaboration with NGOs.
Availability to pain relieving medication especially Morphine:
- Meetings were held with FDA officials to get Morphine license to Sion site & to get official letter that BAMS doctors can prescribe Morphine in Maharashtra.
- A GR of Govt of Maharashtra related to BAMS doctors prescribing allopathic medicines was obtained.
- Jawhar Site has got Morphine license.
Empowerment of children and families for improving Quality of Life:
- Focus Group Discussions have been conducted to have an understanding of needs, issues and psychosocial aspects of children and families
- Various programs were arranged in co-ordination with Sion and Tata Hospital involving children and families.(Support group, Christmas Party)
- Networking with orphanages and other NGOs was strengthened and children were referred for behavioural, psychological and medical problems.

November 2011: The first group of nurses, doctors and Medical officers receive a certificate after doing the one week introduction to children's palliative care course in Lilongwe, Malawi.
Why did ICPCN become involved in this project?
HIV/AIDS continues to have a staggering impact on children. UNAIDS estimates that there are over 2.1 million children under the age of 15 living with HIV/AIDS, the majority of whom were infected by vertical transmission of the virus from parent to child. All told, over 280,000 children die of AIDS each year, and in some countries the epidemic accounts for as many as half of all deaths among children under five.
The palliative care approach responds to the holistic needs of these children living with a life-threatening illness such as HIV and AIDS, to relieve suffering and ensure quality of life and to address their physical, psychological, social, and spiritual needs.
What is the need?
The worldwide response to the paediatric AIDS epidemic lags far behind international commitments. Mothers and children impacted by the epidemic continue to face widespread scarcity of prevention and treatment services, particularly in countries with the highest burdens of maternal and paediatric HIV infection. This is unacceptable when there is treatment available that can prevent HIV transmission from mother to child. In 2007, approximately one million HIV positive pregnant women gave birth without access to these services worldwide and nearly 400,000 infants were born HIV-positive. There were nearly two million children under the age of 15 living with HIV at the end of 2007, the vast majority of whom were infected through vertical transmission from their mothers.
Treatment options for children have expanded, and the number of children on antiretroviral therapy (ART) has increased rapidly, from 75,000 children in 2005 to 198,000 children in 2007. However, the majority of children on treatment are over the age of four, and 50% of HIV-infected infants die before their second birthday. (Global AIDS Alliance: Empowering Health Workers with new Technologies to End Paediatric HIV/AIDS. April 2009)
Most children living with HIV and AIDS live in resource-poor countries and in poverty. Diagnosis, treatment and care support is often difficult to access as services are far from the child’s home and the family may not have the financial resources for transport. Effective care for children maintains them in their homes and communities, is family-centred and provides ongoing support. Two-thirds of all people infected with HIV live in sub-Saharan Africa.
Palliative care can be provided alongside anti-retroviral therapy to improve compliance to the drugs and ensure that the child is cared for holistically. Whilst the need for palliative care for every child with a life-limiting or life-threatening condition such as HIV/AIDS, cancer, neuro-degenerative conditions and severe disabilities is great, services providing palliative care to these children are largely situated in developed countries.
The Maharashtra District of India
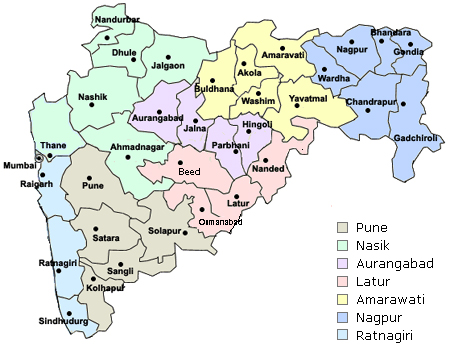
Why were Malawi and India chosen?
Malawi and the Maharashtra District of India were chosen for this project because while both have a high HIV prevalence rate and infant mortality rate, they also have existing paediatric palliative care programmes which can be strengthened and expanded and national palliative care associations willing to support the process. The sites chosen for the project are the Umodzi project at Queen Elizabeth Central Hospital in Blantyre, Malawi, and the Tata Memorial Hospital in the Maharashtra District of India.
Malawi
930 000 people living with HIV /AIDS
11,9 % incidence of HIV
91 000 children living with HIV/AIDS
7th lowest GDP per head
14th lowest on the human development index 43.7
High Infant mortality of 89.4
India – Maharashtra district
2.4 million living with HIV/AIDS
55 506 children with HIV/AIDS
The 4th highest incidence of HIV/AIDS in India
Long Term Goals:
Through the introduction of this project in Malawi and India, the ICPCN is looking to achieve the following long term goals:
- To strengthen existing palliative care services for children.
- To develop palliative care services for children through integration into at least three existing projects and organisations in each country.
- To integrate palliative care policies for children into national palliative care associations.
- To improve access to HAART, palliative care drugs and pain medication for children.
- To advocate for the expansion of palliative care for children and its integration into government policies and national, regional and local health care systems.
- To educate health care practitioners in paediatric palliative care using a curriculum appropriate for developing countries.
- To develop materials on children's palliative care in local languages.
- To foster and protect the rights of children to life, education and sound health
Description of what the project will do and achieve:
- Advocacy to expand palliative care for children and integrate it into health systems.
- Strengthening of existing palliative care for children in both countries.
- Education of health care practitioners using a new curriculum for developing countries.
- Support to development through ICPCN.
- Virtual Children's Palliative Care resource for all developing programmes.
- Development of in-country materials in local languages.
- M&E and write up of development for use in other countries.
- In-country coordinators.
- Protection of the rights of children to life, education and health.
- Support for women and girls caring for children.
- Involvement of men and boys in Children's Palliative Care.
- Advocacy at global level through ICPCN with WHO, UNICEF, and other major stake-holders.
- Strengthen partnerships and the international and regional networks through ICPCN.
- Involve civil society organizations in each country in development and advocacy, and supporting government policy.
- Indication of the impact the project will have on the beneficiaries (i.e. children).
- Improve access to ART, palliative care and palliative care drugs.
- Improve life-expectancy and quality of life.
- Treatment by professionals trained in Children's Palliative Care.
- Relieve pain and suffering
- Protect children’s rights